Multisystem Atrophy - Parkinsonian Type (MSA-P)¶
Summary
- MSA-P is a neurodegenerative disorder characterised by parkinsonian features, autonomic dysfunction, and cerebellar ataxia
- Pathologically, it involves α-synuclein accumulation in oligodendrocytes and neuronal loss in multiple brain regions
- Imaging reveals characteristic patterns of atrophy and signal changes in the basal ganglia, cerebellum, and brainstem1
Pathophysiology¶
- Accumulation of α-synuclein in glial cytoplasmic inclusions (GCIs) in oligodendrocytes
- Neuronal loss and gliosis in:
- Substantia nigra
- Striatum
- Globus pallidus
- Pontine nuclei
- Inferior olivary nuclei
- Cerebellar Purkinje cells
- Degeneration of autonomic nuclei in the brainstem and spinal cord
Demographics¶
- Typical onset: 50-60 years of age
- Slight male predominance (1.3:1)
- Estimated prevalence: 3-4 per 100,000 population
- More common in Caucasian populations
Diagnosis¶
- Clinical features:
- Parkinsonism (bradykinesia, rigidity, postural instability)
- Autonomic dysfunction (orthostatic hypotension, urinary incontinence, erectile dysfunction)
- Poor response to levodopa therapy
- Diagnostic criteria:
- Probable MSA-P: Parkinsonism + autonomic failure/urinary dysfunction
- Possible MSA-P: Parkinsonism + autonomic dysfunction or cerebellar syndrome
Imaging¶
- MRI findings:
- Putaminal atrophy with T2 hypointensity
- "Hot cross bun" sign in pons (T2/FLAIR hyperintensity)
- Cerebellar atrophy
- "Putaminal rim" sign (T2 hyperintensity at lateral putaminal border)
- DaTSCAN:
- Reduced striatal dopamine transporter uptake
- FDG-PET:
- Hypometabolism in striatum, brainstem, and cerebellum
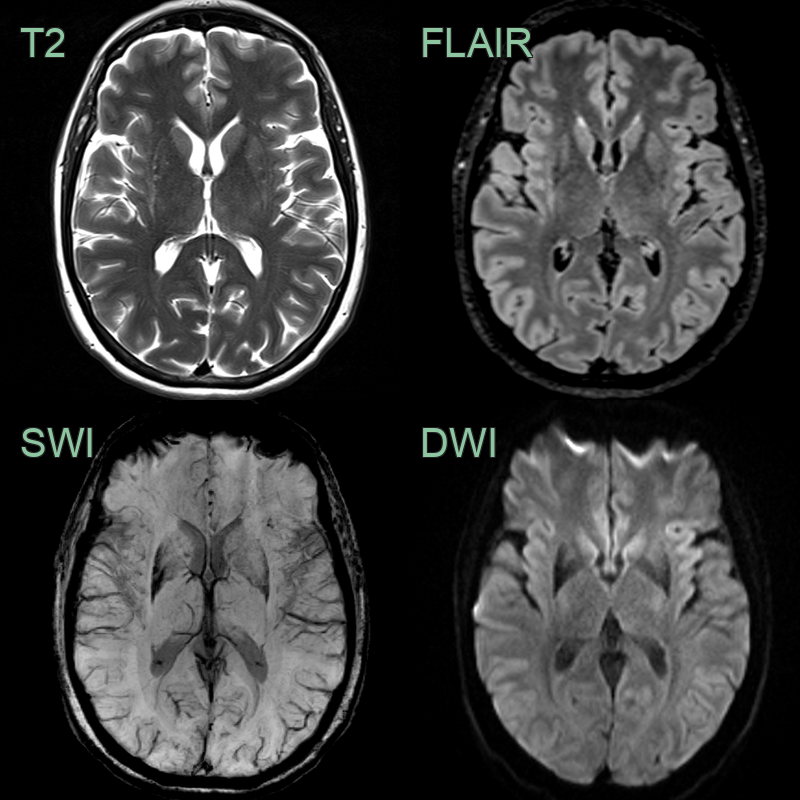
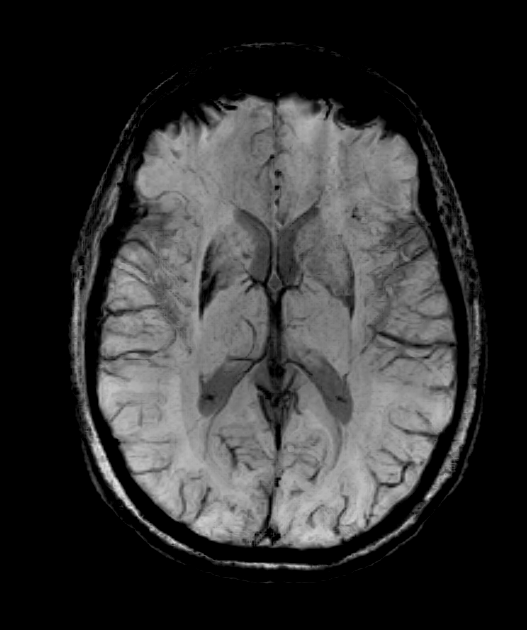
- 55-year-old female with left sided parkinsonism and orthostatic symptoms.
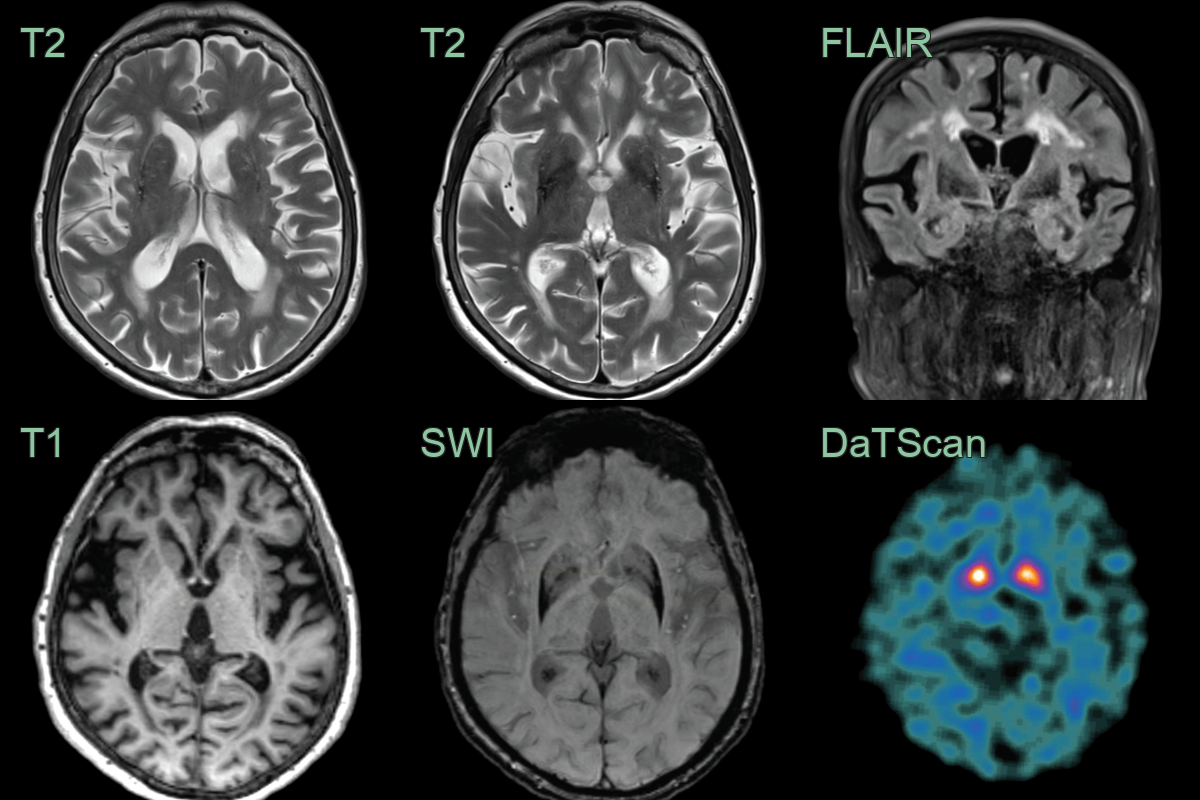
- 80-year-old patient presented with asymmetric parkinsonism (left > right) with freezing and early falls with poor response to levodopa.
- MRI showed putaminal atrophy, susceptibility artefact and T2-hyperintensity along the lateral aspect of the putamina.
- DaTscan showed markedly reduced tracer uptake in the putamina bilaterally.
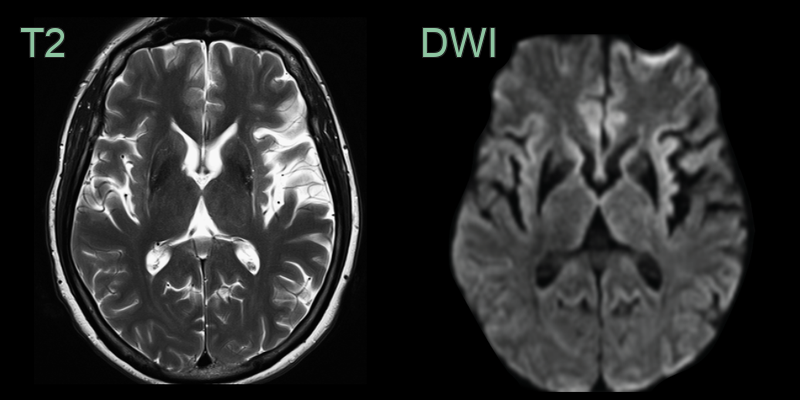
- 60-year-old patient with a bilateral tremor.
- T2 weighted imaging shows the lateral rim sign and mild putaminal volume loss.
- While SWI was not performed, low signal was seen in the putamina on EPI DWI, which is sensitive to susceptibility artefact.
Treatment¶
- Symptomatic only; parkinsonism responds poorly to levodopa
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Parkinson's disease | Normal putamen and preserved nigrosome-1 sign is more typical; MSA-P shows putaminal atrophy, T2 hypointensity and a lateral rim |
| Progressive supranuclear palsy | Midbrain atrophy ("hummingbird"/"morning glory"); superior cerebellar peduncle atrophy |
| Corticobasal degeneration | Asymmetric perirolandic cortical atrophy |
| MSA-cerebellar type | Predominant pontocerebellar atrophy with "hot cross bun" sign |
| Vascular parkinsonism | Basal ganglia lacunes and confluent small vessel disease |
-
Krismer et al. Multiple system atrophy: advances in pathophysiology, diagnosis, and treatment. 2024. The Lancet. Neurology - Open in new tab. ↩