Progressive Supranuclear Palsy (PSP)¶
Summary
- Progressive neurodegenerative disorder characterised by postural instability, supranuclear gaze palsy, and cognitive decline
- Pathologically defined by accumulation of tau protein in neurons and glial cells
- Imaging shows midbrain atrophy with the 'hummingbird' sign in the sagittal plane1
Pathophysiology¶
- Accumulation of hyperphosphorylated tau protein in neurons and glial cells
- Neuronal loss and gliosis in affected areas
- Familial cases associated with MAPT gene mutations
Demographics¶
- Typically affects individuals over 60 years of age
- Estimated prevalence of 5-6 per 100,000
- No clear ethnic or geographical predisposition
Diagnosis¶
- Clinical diagnosis based on:
- Progressive balance and gait disturbances
- Supranuclear gaze palsy, particularly affecting vertical eye movements
- Cognitive decline and behavioural changes
- Supportive features:
- Axial rigidity
- Dysphagia and dysarthria
- Frontal lobe signs
- Imaging shows excessive midbrain volume loss
- Definitive diagnosis requires neuropathological confirmation
Imaging¶
- Midbrain atrophy is the hallmark:
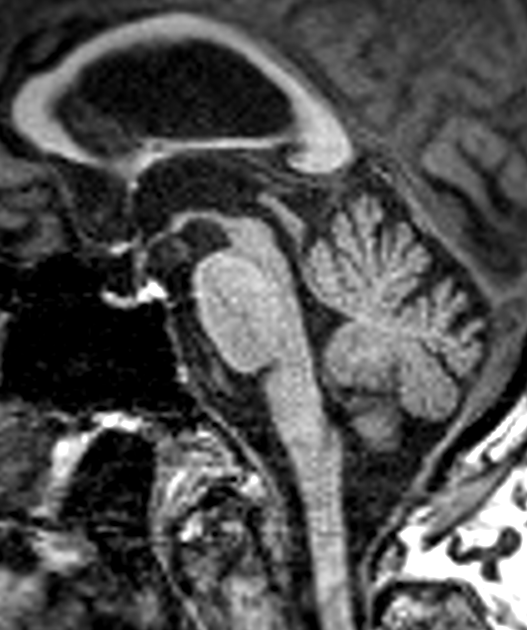
- Sagittal: flattening/concavity of the superior midbrain ("hummingbird" or "penguin silhouette" sign) and a reduced midbrain-to-pons ratio
- Axial: concave lateral midbrain margins ("morning glory" sign)
- Superior cerebellar peduncle atrophy; third ventricle/interpeduncular cistern widening
- The MR parkinsonism index combines these measurements to support the diagnosis

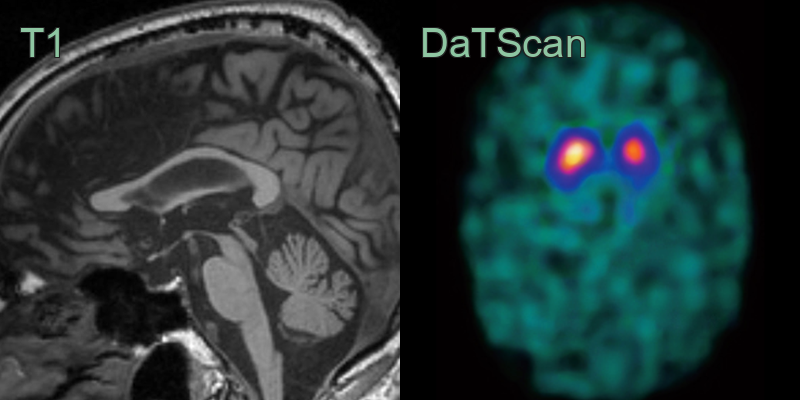
- 75-year-old patient with postural instability and supranuclear palsy.
- The midbrain tegmentum is atrophic causing a flattened superior border.
- The DaTscan shows reduced tracer uptake in the putamina (particularly on the right).
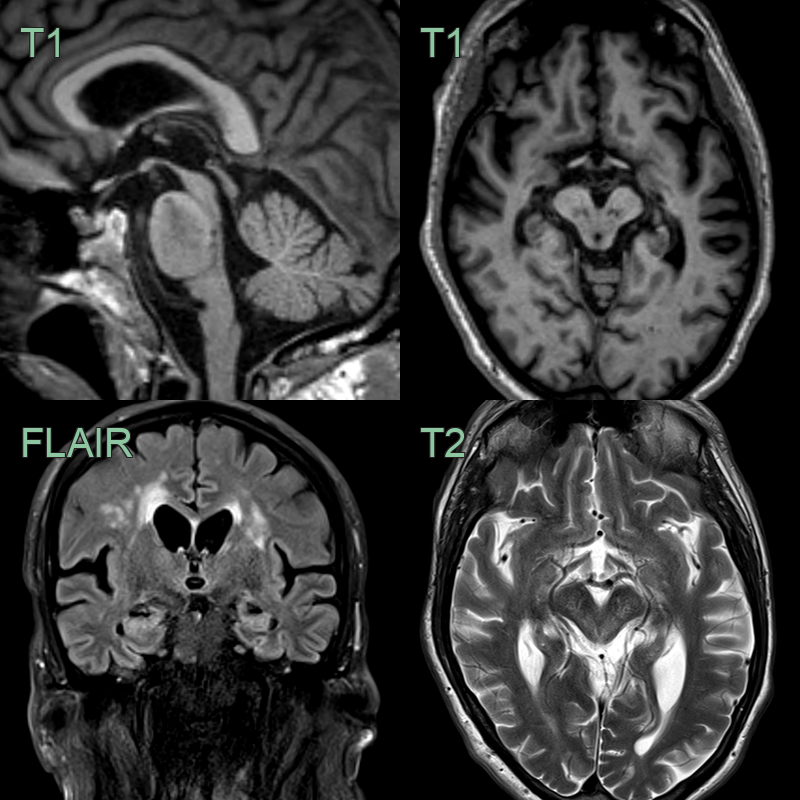
- 65-year-old patient presented with instability, free falls, and a vertical gaze palsy.
- MRI showed marked atrophy of the pons.
- DaTscan showed loss of normal tracer uptake in both corpora striata.
- 60-year-old patient presented with poor balance, multiple falls, and rigidity. Initially diagnosed with Parkinson's disease, there was a poor response to levodopa.
- MRI showed marked midbrain atrophy (as well as a moderate burden of small vessel disease).
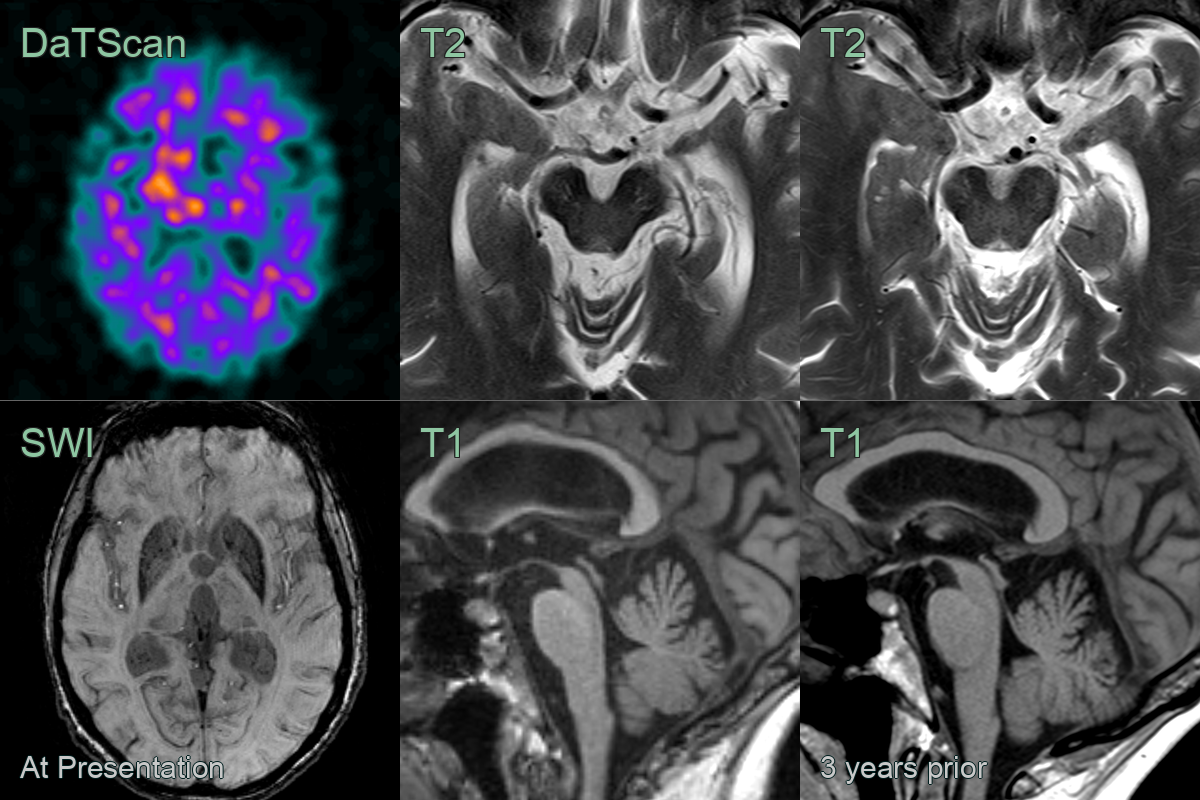
- 70-year-old patient presented with parkinsonism.
- MRI showed marked atrophy of the midbrain over a three year period.
- DaTscan showed high background uptake and with loss of the normal uptake in the striatum.
Treatment¶
- No disease-modifying therapy; levodopa is usually poorly responsive
Differential diagnosis (midbrain/atrophy patterns)¶
| Imaging differential | Differentiating feature |
|---|---|
| Parkinson's disease | Preserved midbrain volume; nigrosome-1 loss on SWI |
| MSA — parkinsonian type | Putaminal atrophy with a lateral rim; "hot cross bun" pons rather than midbrain atrophy |
| Corticobasal degeneration | Asymmetric perirolandic cortical atrophy |
| Normal pressure hydrocephalus | Ventriculomegaly with DESH; preserved midbrain |
-
Boxer et al. Advances in progressive supranuclear palsy: new diagnostic criteria, biomarkers, and therapeutic approaches. 2017. The Lancet. Neurology - Open in new tab. ↩