Vestibular Aqueduct Dehiscence¶
Summary
- A "third window" lesion in which the bone separating the vestibular aqueduct from an adjacent high-riding jugular bulb is deficient
- Presents with pulsatile tinnitus and pressure- or sound-induced vertigo
- Diagnosed on high-resolution temporal bone CT1
Pathophysiology¶
- Dehiscence creates an abnormal "third window" into the labyrinth, dissipating acoustic/pressure energy and abnormally stimulating the vestibular system
- Typically occurs where a high-riding or diverticular jugular bulb erodes the vestibular aqueduct
Diagnosis¶
- Pulsatile tinnitus, sound- or pressure-induced (Tullio) vertigo, sometimes a low-frequency air–bone gap
- Clinically overlaps with other third-window lesions such as superior semicircular canal dehiscence
Imaging¶
- High-resolution temporal bone CT is the key test:
- Focal bony defect between the vestibular aqueduct and the jugular bulb
- Usually an associated high-riding or dehiscent jugular bulb
- Reformatting along the plane of the aqueduct avoids overcalling dehiscence from partial-volume averaging
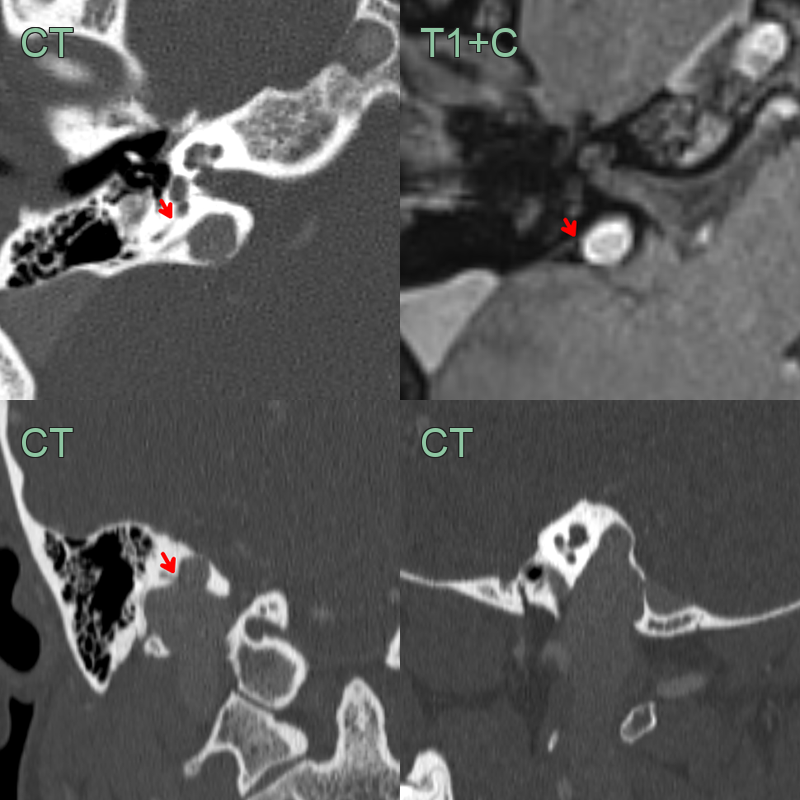
- A 40-year-old patient presented with constant right sided pulsatile tinnitus and intermittent vertigo.
- CT showed a communication/dehisence of the right vestibular aqueduct (red arrows) onto a high-riding jugular bulb.
Treatment¶
- Usually conservative; surgical resurfacing is reserved for disabling symptoms once other causes are excluded
Differential diagnosis¶
| Imaging differential | Differentiating feature |
|---|---|
| Superior semicircular canal dehiscence | Bony defect over the superior semicircular canal rather than the vestibular aqueduct |
| Sigmoid sinus dehiscence | Absent bone over the sigmoid plate — a venous cause of pulsatile tinnitus |
| Enlarged vestibular aqueduct | Widened aqueduct (>1.5 mm) causing sensorineural hearing loss, without a jugular bulb defect |
| Glomus tympanicum / jugulare | Enhancing vascular middle-ear or jugular foramen mass |
-
Guarnizo et al. High jugular bulb with a diverticulum and vestibular aqueduct dehiscence: an anatomical variant to be aware in patients with hearing loss. 2022. Surgical and radiologic anatomy : SRA - Open in new tab. ↩