Intracranial Aneurysm¶
Summary
- Focal dilatation of cerebral artery wall, typically at branching points
- Risk of rupture leading to subarachnoid haemorrhage
- Diagnosis primarily through imaging, treatment options include surgical clipping and endovascular coiling1
Pathophysiology¶
- Weakening of arterial wall due to haemodynamic stress and structural abnormalities
- Common locations: anterior communicating artery, posterior communicating artery, middle cerebral artery bifurcation
- Risk factors for formation:
- Genetic predisposition (e.g., polycystic kidney disease)
- Hypertension
- Smoking
- Excessive alcohol consumption
Demographics¶
- Prevalence: 3-5% of general population
- More common in females (1.6:1 ratio)
- Peak incidence of rupture: 40-60 years old
- Higher prevalence in certain populations:
- Finnish and Japanese populations
- First-degree relatives of patients with intracranial aneurysms
Diagnosis¶
- Often asymptomatic until rupture
- Symptoms of unruptured aneurysms:
- Headache
- Cranial nerve palsies
- Seizures
- Ruptured aneurysm presentation:
- Sudden, severe headache ("thunderclap headache")
- Neck stiffness
- Photophobia
- Altered consciousness
- Diagnostic tools:
- CT angiography (CTA)
- Magnetic Resonance Angiography (MRA)
- Digital Subtraction Angiography (DSA)
Imaging¶
- CT without contrast:
- Acute subarachnoid haemorrhage: hyperdense blood in subarachnoid spaces
- Calcification in aneurysm wall
- CTA:
- High sensitivity (77-97%) and specificity (87-100%) for aneurysms >3mm
- Allows 3D reconstruction for surgical planning
- MRA:
- Time-of-Flight (TOF) technique: high sensitivity for aneurysms >3mm
- Contrast-enhanced MRA: improved detection of small aneurysms
- DSA:
- Gold standard for diagnosis and characterization
- Allows dynamic assessment of flow and collateral circulation
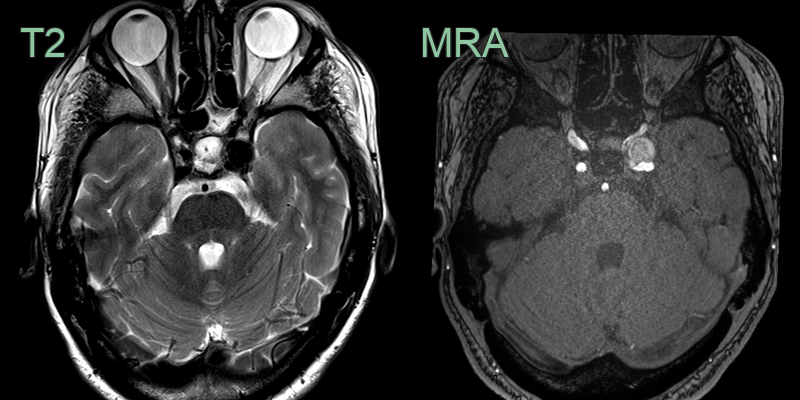
- An MRI in a patient with a longstanding left lateral rectus palsy showed a 1.2 cm cavernous ICA aneurysm interfering with the left abducens nerve.
- The left lateral rectus was atrophic.
Treatment¶
- Ruptured aneurysms are secured by endovascular coiling/flow diversion or surgical clipping
- Small unruptured aneurysms are often surveilled; rupture risk rises with size, posterior circulation location and growth
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Arteriovenous Malformation | Presence of feeding arteries and draining veins on angiography |
| Cavernous Malformation | Characteristic "popcorn" appearance on MRI |
| Meningioma | Extra-axial location and dural tail sign on MRI |
| Pituitary Adenoma | Sellar/suprasellar location; no flow voids; enhances homogeneously |
| Glioma | Infiltrative appearance with surrounding oedema; no flow void or arterial origin |
| Metastasis | Multiple lesions at grey-white junction; no flow void; ring or nodular enhancement |
| Cerebral Abscess | Ring-enhancing lesion with restricted diffusion on MRI |
| Thrombosed Giant Aneurysm | Layered appearance on MRI with varying signal intensities |
| Developmental Venous Anomaly | Characteristic "caput medusae" appearance on contrast-enhanced imaging |
| Capillary Telangiectasia | Faint enhancement on MRI without mass effect |
-
Allaw et al. A Review of Intracranial Aneurysm Imaging Modalities, from CT to State-of-the-Art MR. 2025. AJNR. American journal of neuroradiology - Open in new tab. ↩